|
|
 |
 |
 |
|
 |
|
 |
|
D. de Ziegler, Dept of Ob Gyn, Hopital de Nyon, Switzerland. ASRM 2003, San Antonio, TX
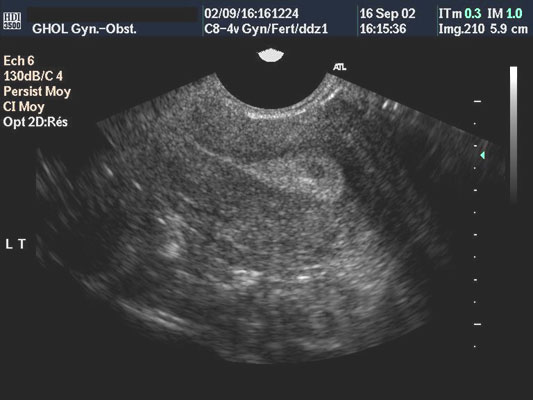
Objective - In pregnancy, the amniotic fluid serves as an intrauterine contrast enhancer, providing a negative or "black" sonic interface. This plays a crucial role in the remarkable quality of ultrasound images obtained in obstetrics. In the non-pregnant uterus, the uterine cavity is not as easily visualized due to the lack of a contrasting interface. Hence, normal and pathological images (polyps, sub-mucosal fibroids) are often insufficiently sharp to permit a definitive diagnosis. Efforts to improve the quality of images of the non-pregnant uterus have led to negative ("black") or positive ("white") contrast medium being instilled in the uterine cavity while the echographic evaluation, known as hysterosonography (HSG), is performed. Unfortunately HSG, which provides images of excellent quality, is cumbersome, time consuming and requires more than 1 person to perform. To achieve the quality of uterine images obtained with HSG while retaining the simplicity and great ease of use of regular vaginal ultrasounds, a phase-shifting uterine contrast medium (PSCM) has been developed. When instilled in the uterus with a regular embryo transfer catheter, the medium is thick and moderately distends the cavity. The PSCM, which has the sonic characteristics of water, provides a negative or "black" contrast that allows excellent visualization of structures protruding in the cavity, such as endometrial polyps and/or sub-mucosal fibroids. Endowed with phase-shifting characteristics, the PSCM subsequently liquefies as its temperature rises and reaches body temperature. Once fluid, uterine distension stops and the PSCM is expelled. Design - Prospective pilot feasibility study in infertile women and women with dysfunctional endometrial bleeding (DUB). Materials and Methods - 53 women consulting for infertility (n=27) or DUB (n=26) were studied. After a conventional vaginal ultrasound was performed, all underwent contrast ultrasound examination. For this, 3-7cc of PSCM was infused in the uterine cavity using a 3.5 Frydman embryo transfer catheter. The uterine catheter was then removed and another vaginal ultrasound was performed. Results - In all women, the uterine cavity remained distended for > 3 minutes, leaving a >3.5 mm thick "black" interface in the uterine cavity. In all patients uterine distension and medium had disappeared after 10 minutes. In 21 of 26 women presenting with DUB, contrast ultrasound revealed an intrauterine pathology that was subsequently confirmed by hysteroscopy and histology. In 14 of them, conventional vaginal ultrasound had not provided a definitive diagnosis. Conclusion - This reports the development of a novel PSCM, which generates a time-limited moderate distension of uterine cavity, providing a sono-transparent ("black") inter-phase. This offers "contrast ultrasound" vision, which greatly facilitates the positive diagnosis of intrauterine structures such as polyps and fibroids. Contrast ultrasound of the uterus using PSCM may revolutionize uterine echography, as it provides images of hysterosonography quality, while retaining ease of use and the simplicity of general trans-vaginal ultrasounds. |